Hypoplastic Left Heart Syndrome, HLHS
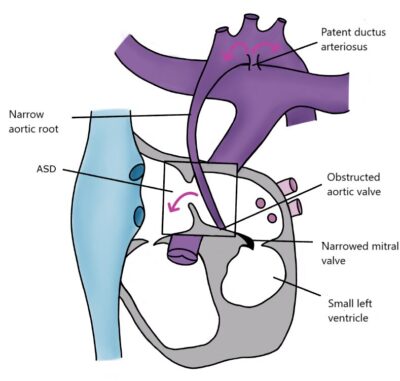
Hypoplastic Left Heart Syndrome (HLHS) means that the underdeveloped left ventricle is so small that it cannot pump enough blood. The mitral and/or aortic valves may be absent or function poorly. The entire systemic circulation, including the coronary arteries, depends on an open ductus arteriosus. If left untreated, the closure of the ductus arteriosus will result in the patient’s death.
Today, the majority of HLHS patients are diagnosed before birth. Confirming the diagnosis before birth provides better preparation to assist the child immediately after delivery. If the heart defect is not detected before birth, HLHS is usually diagnosed within the first few days of life.
Treatment and prognosis
The underdeveloped left side of the heart cannot be repaired to function as a normal pumping heart. Children with HLHS are typically treated with a three-stage palliative surgical series. The first stage, the Norwood procedure, is performed when the newborn is about one week old. The main pulmonary artery is divided, and its base is connected to the aortic arch, and the atrial septum is opened. Blood is directed to the lungs from the aorta or the right ventricle using a vascular graft. The second surgery is performed at around six months of age. The superior vena cava is connected to the pulmonary artery, allowing low-oxygen blood from the upper body to flow to the lungs under venous pressure. The shunt created in the previous surgery from the aorta or right ventricle to the pulmonary artery is closed. The third surgery is typically performed at around 3-4 years of age, during which blood from the inferior vena cava is also directed to the pulmonary artery. In simplified terms, a single-ventricle heart (UVH) is created for the child by rerouting major blood vessels in three different stages.
Cerebral blood flow is already below normal before birth. Patients undergo three major heart surgeries, each carrying risks that may impact their later development. In a Finnish study, at the age of five, patients exhibited below-average physical performance. Approximately 50% had motor developmental delays, and two-thirds of patients had neurological issues. Among them, about 26% had significant neurological problems, and more than 40% had milder neurological issues.
In rare cases, it may be deemed that surgery is not advisable. This might occur if the child is very premature or underweight, has another condition with a poor prognosis, or if the patient’s condition cannot be stabilized before surgery. The decision is always made on a case-by-case basis after thorough consideration. In practice, nearly all HLHS patients are candidates for surgical intervention.
HLHS patients have permanently reduced physical capacity, and heart failure medications have not been shown to be beneficial for heart failure resulting from this defect. Patients require lifelong cardiac monitoring.